Excision of Calcific Tendinitis Surgery
Overview
Calcific tendinitis is a painful condition affecting the shoulder. It is more common in women, aged between 25 and 55 years old. Whilst, calcium deposits are commonly found around the shoulder, a small proportion of people will have inflammation and pain from these. Most of the time, these symptoms settle spontaneously, and do not require surgical treatment.
Indications for surgery
Surgery is reserved for patients with pain and calcific deposits that have not settled with injections and physiotherapy. It is more common in patients with larger deposits in their shoulder tendons. Surgery is performed with keyhole techniques, and simply remove the calcium deposits.
Pre-surgery tests and assessment
Before any keyhole surgery to the shoulder, a variety of assessments and tests, such as X-rays, and a MRI scan are performed. Dr. Rashid will assess your calcium deposit size and location carefully. Occasionally, a tendon tear is also associated with the calcium deposits, and Dr. Rashid will discuss with you how this will be repaired.
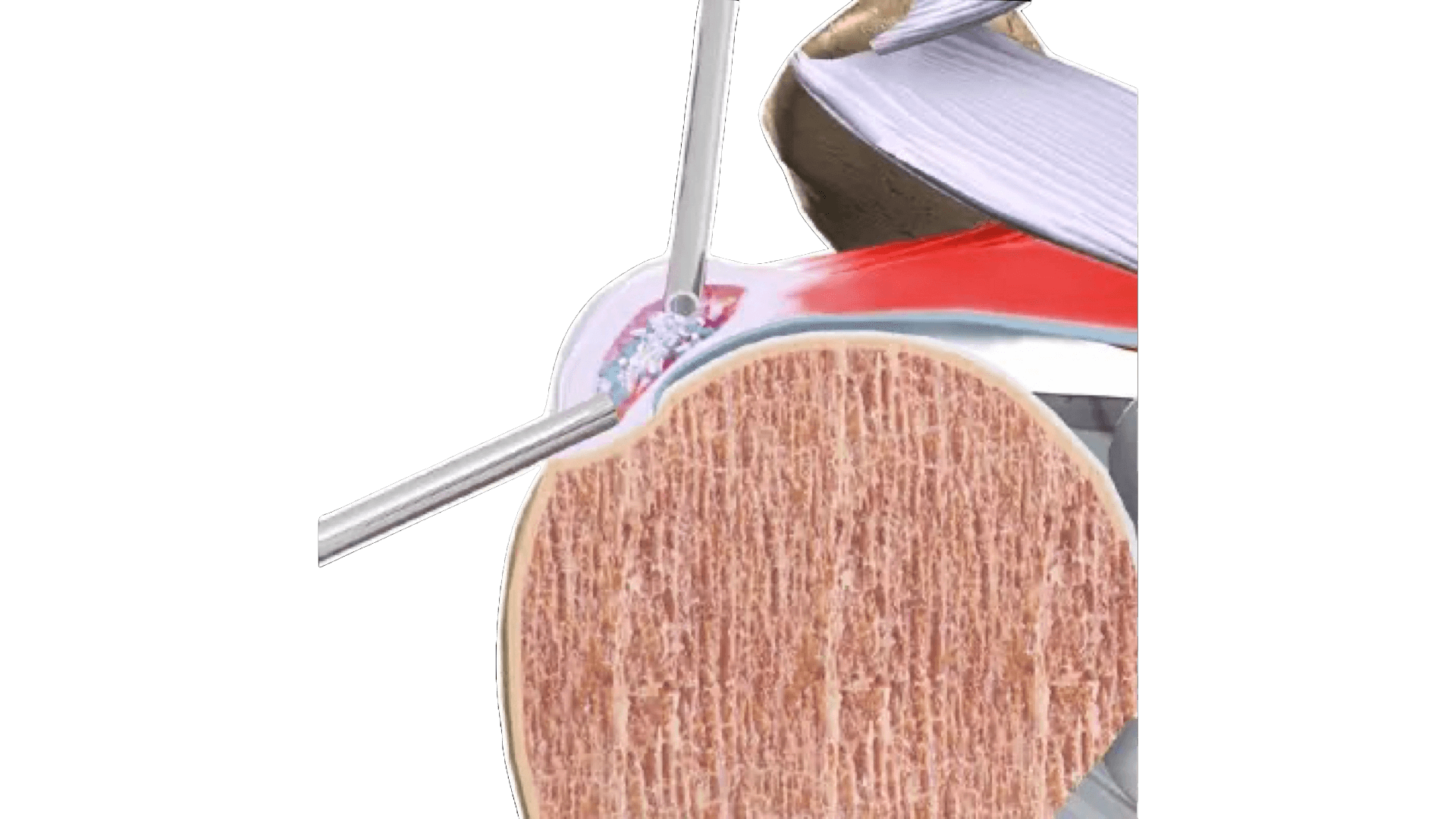
Procedure Details
Under general anaesthesia, you will be positioned onto your side and your arm will be placed in a special arm holder. After sterilising the skin with a cleaning solution, a keyhole camera is inserted into your shoulder. The inflamed areas and calcium are then located. Then, using a scalpel and a radiofrequency device the inflamed areas are removed and the calcium is excised. After removing the calcium from the tendon, Dr. Rashid will then reassess the defect left behind within your tendon. If this is significant, it may require repair or a special patch, made from bovine collagen, placed over the defect to allow it to heal. The skin incisions are closed with stitches that are absorbable and buried under the skin. Dressings and a sling are then applied. This type of surgery typically takes less than one hour.
Risks and Complications
The risks of calcium excision surgery are not common. These include infection, stiffness, tendon injury, and nerve injury (very rare). Dr. Rashid has carefully trained over many years to perform this operation and can do so safely and effectively. Dr. Rashid also uses a cortisone steroid injection at the end of the surgery to reduce the inflammation response from the operation, helping manage pain and reducing the risk of stiffness.
Recovery and rehabilitation
Recovery following this type of surgery involves discarding your sling as soon as you are comfortable (usually in the first few days), and commencing early movement and stretching exercises to maintain your range of motion. If a repair of the tendon is performed, then Dr. Rashid will outline a protocol for rehabilitation that may include a few weeks in the sling at the beginning. Physiotherapy is helpful to ensure you regain your motion, function, and strength of the shoulder. Pain relief is often appreciated in the first month.
Expected Outcomes
Most people choose this surgery to gain quick results and return to normal activities sooner than if they wait for their inflamed tendon and calcium to resolve naturally. Most people are able to return to tennis, golf, swimming, weightlifting, and physical labour between 1 and 3 months after surgery. Dr. Rashid will follow your progress closely to ensure that your shoulder is rehabilitating well over time. Most people can return to work, including driving with 2 weeks. Most people will successfully return to full movement and function within a short amount of time (typically 3 months). This is mostly determined by how well you do your stretching and physical therapy exercises after surgery.
About the Author

Mustafa Rashid
Dr. Mustafa Rashid is an award-winning, well published superspecialised surgeon from the UK, specialising in shoulders